Ingat lagi saya bercerita pasal khadijah yang kena amik darah lagi masa previous check up kat hospital untuk check bone density ke apa test. Yang pasti berkaitan dengan ketumpatan tulang dia lah, berkaitan juga dengan penyakit rickets ni. Setelah beberapa page membacanya, maka ummi dapatlah pemahaman tentang apa sebenarnya yang Doc tu cakapkan.
Rickets is an entity in which mineralization is decreased at the level of the growth plates, resulting in growth retardation and delayed skeletal development. Osteomalacia is found within the same spectrum, affects trabecular bone, and results in undermineralization of osteoid bone. By definition, rickets is found only in children prior to the closure of the growth plates, while osteomalacia occurs in persons of any age. Any child with rickets also has osteomalacia, while the reverse is not necessarily true.1,2,3

Anteroposterior and lateral radiographs of the wrist of an 8-year-old boy with rickets demonstrates cupping and fraying of the metaphyseal region.

Radiograph in a 4-year-old girl with rickets depicts bowing of the legs caused by loading.
Melihat pada keadaan fizikal khadijah saat ini, memang dia tiada tanda-tanda seperti di atas. Itu dari mata kasarnya lah. Dan khadijah nampak selesa dengan keadaan dia sekarang, merangkak dan mula berdiri memegang sesutu untuk bertatih. Cuma dia masih takut-takut untuk lepas tangan berdiri sendiri.
sambungan..Because rickets results from a metabolic disturbance, the underlying disease should be diagnosed. The causes of rickets can be classified into 11 main categories:- Vitamin D deficiency
- Dietary deficiency
- Deficient endogenous synthesis
- Gastrointestinal tract disorders
- Small intestine diseases with malabsorption
- Partial or total gastrectomy
- Hepatobiliary disease
- Chronic pancreatic insufficiency
- Disorders of vitamin D metabolism
- Hereditary - Pseudovitamin D deficiency or vitamin D dependency (types I and II)
- Acquired
- Use of anticonvulsants
- Chronic renal failure
- Acidosis
- Distal renal tubular acidosis (classic or type I)
- Secondary forms of renal acidosis
- Ureterosigmoidostomy
- Drug-induced disease
- Chronic acetazolamine ingestion
- Chronic ammonium chloride ingestion
- Chronic renal failure
- Phosphate depletion
- Dietary - Low phosphate intake plus ingestion of nonabsorbable antacids
- Hereditary - X-linked hypophosphatemic rickets or adult-onset vitamin D–resistant hypophosphatemic osteomalacia
- Acquired - Sporadic hypophosphatemic osteomalacia (phosphate diabetes), tumor-associated (oncogenous) rickets, osteomalacia, neurofibromatosis, and fibrous dysplasia
- Generalized renal tube disorders
- Primary renal tube disorders
- Renal tube disorders associated with systemic metabolic abnormality
- Cystinosis
- Glycogenosis
- Lowe syndrome
- Systemic disorder with associated renal disease
- Hereditary - Inborn errors (Wilson disease, tyrosinemia) and neurofibromatosis
- Acquired - Multiple myeloma, nephrotic syndrome, and kidney transplantation
- Intoxication-related - Cadmium, lead, outdated tetracycline
- Primary mineralization defects
- Hereditary
- Acquired
- Diphosphonate treatment
- Fluoride treatment
- States of rapid bone formation with or without a relative defect in bone resorption
- Postoperative hyperparathyroidism with osteitis fibrosa cystica
- Osteopetrosis
- Defective matrix synthesis - Fibrogenesis imperfecta ossium
- Miscellaneous
- Magnesium-dependent conditions
- Axial osteomalacia
- Parenteral alimentation
- Aluminum intoxication
- Isofosfamide treatment
Age - By definition, rickets occurs only in children whose growth plates have not closed. The growth plates close at the end of puberty, at approximately age 17 years in females and age 19 years in males.
- Premature neonates are especially at risk because their requirements for vitamin D, calcium, and phosphate are higher than those in full-term neonates.
Clinical findings are related to the involved skeletal site.
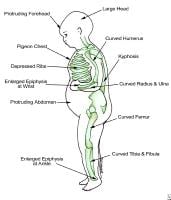
Findings in patients with rickets.
- Head
- Skull - Craniotabes may occur, in which the bones of the skull soften and flattening of the posterior skull can be seen. These effects may be transient or permanent. Another feature is the prominence of the frontal bones and the major foramen, resulting in frontal bossing or a prominent, sometimes square, forehead (caput quadratum).
- Teeth - Teeth may erupt later than normal because of undermineralization. Enamel can be of poor quality, resulting in caries. --- setakat ni khadijah hanya ada 4 batang gigi, dua atas dua bawah. Consider lambat tumbuh ke?
- Thorax
- Rachitic rosary - The enlarged ends of the ribs, resembling beads, can be palpable and visible at the costochondral junction. As a result, the sternum can become more prominent, leading to a pigeon breast or pectus carinatum appearance.
- Harrison groove - The groove is a semicoronal impression over the abdomen at the level of the insertion of the diaphragm, which can be seen in rickets.
- Spine - A mild to more pronounced scoliosis may be seen as a result of rickets.
- Pelvis - A prominent promontory can be found, and the anteroposterior (AP) diameter of the pelvis can shrink as a result of scoliosis. If this persists in girls, it can cause complications later in life during childbirth.
- Extremities
- Arms
- Bowing of the long bones, as a reaction to greenstick fractures, results from concurrent osteomalacia.
- Thickening of the wrist at the level of the epiphysis is not visible radiographically, since the lesion consists of cartilage, although fraying and cupping of the metaphysis is evident.
- Legs
- Bowing of the long bones (genu varum)as a result of weight bearing is typical.
- Anterior bowing of the tibia (saber shin deformity) may occur.
- Development of knock-knees (genu valgum) may occur because of displacement of the growth plates during active disease.
- Thickening at the level of the ankle may occur, identical to the process in the wrist.
- Ligaments and muscles - Laxity in the ligaments is increased, and muscle tone is decreased. This combination leads to a delay in motor development.
Preferred Examination
Plain radiography of the affected bones is the preferred examination. The distal radius and ulna typically demonstrate rachitic lesions early on radiographs. In preterm neonates and young infants, radiographs of the knee may be more reliable than those of the wrist.
Sumber:
klik sini.
Saya ingatkan ricket ni hanya mempunyai tulang kaki yang membengkok ke dalam seperti gambar di atas tu, rupanya ia boleh juga dalam bentuk dan keadaan lain. Banyak juga tu yang masih belum dapat saya pastikan adakah khadijah ada tanda-tandanya. Kena balik check dan yang pasti, ia bukan perkara boleh dipandang ringan. It will affect her whole life kalau sekiranya dia ada potential untuk masalah tersebut dan tidak dirawat sejak mula. Nervous ummi membacanya ni. Btw, Paed dia ada cakap kalau ada apa-apa dia akan call, tapi takde pula call setakat ni, harapnya semua ok lah tu.
3 comments:
Salam mirah...hopefully sumanya ok, insya'allah :)
nak kena ambil tahu juga ni though Syafiah tak de la tanda yang nyata. cuma gigi dia kuning sket.
cabaran untuk neonate ni banyakkan. kita kena monitor banyak benda, terutamanya dari segi pemakanannya. tapi insyaAllah as the time goes by, things get better kot...
Fiza, insyaAllah..
K sue, ya memang byk benda nak kena ambil tahu..
Post a Comment